78 years old male with throat pain, cough, breathlessness
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
K.Vyshnavi
Roll No - 70
PATIENT CAME TO THE OPD,WITH THE CHIEF COMPLAINTS OF :
C/O Breathlessness since 7days
C/O Cough since 7days
C/O Throat pain since 3 months
Patient was apparently alright 3months back the he developed throat pain since 3 months, insidious in onset, gradually progressed. Dysphagia positive to both solids and liquids.
C/O Breathlessness since 7 days, insidious in onset, gradually progressive (MMRC GRADE- 2), aggrevated on exposure to cold, seasonal variation present, associated with wheeze, no PND no orthopnea
C/O cough since 7 days which is dry, no seasonal and diurnal variation, continuous, no aggrevating and relieving factors
C/O fever occasionally not associated with chills and rigor, but evening raise of temperature positive.
C/O loss of appetite and loss of weight present
No C/O chest pain, chest tightness,hemoptysis
PAST ILLNESS:
H/O PTB 4 years back confirmed by sputum cbnaat and took ATT for 3 months and discontinued and 2 years back for 6 months
H/O similar complaints in past (3years back)
Inhaler usage present on and off, last usage one day before admission
K/C/O DM and on medication ()
N/K/C/O HTN, Thyroid disorder, CAD, Epilepsy
PERSONAL HISTORY
Appetite -Normal
Diet - Mixed
Sleep - adequate
Bowel and bladder movements -Regular (burning micturition+)
Addictions: 2 packs per day beedi, stopped 10 years back, occasionally alcoholic
Allergies : No allergies
GENERAL EXAMINATION:
Patient is conscious ,coherent , cooperative, thinly Built and mildly Nourished .
He was examined under well lit room with consent taken
VITALS ( on admission)
Temp: 99F
BP : 120/70 mmHg
PR : 130bpm
RR : 20cpm
SpO2: 92%@ RA
Weight- 38kgs
Pallor : absent
Icterus : absent
Cyanosis: absent
Clubbing : absent
Lymphadenopathy : absent
Edema : absent
RS :
INSPECTION:-
URT:
Nose - DNS to right side and left turbinte hypertrophy
Oral cavity- poor oral hygiene, nicotine stained, posterior pharyngeal wall- normal
LRT:
Shape of chest- symmetrical and elliptical
Trails sign negative
Supra clavicular, infra clavicular hollowness - negative
Chest expansion equal on both sides
No crowding of ribs, drooping of shoulders
Wasting of muscles- negative
No usage of accessory muscles on respiration
Spino scapular distance is equal on both sides
Apical impulse - not seen
No kyphosis, scoliosis, sinuses,scars, engorged veins, visual pulsations
PALPATION:-
All inspectory findings are confirmed
Trachea- central, swelling positive in midline
Apex beat is at left 5th ICS, 1 inch medial to mid clavicular line
Tactile vocal fremitus: increased @ Left ICA, MA, INFRA SA, INFRA AA
AP DIAMETER- 19cm
Chest circumference- 73cm
Transverse- 22cm
Rt hemi thorax- 39cm
Lt hemi thorax- 37cm
PERCUSSION -
Direct- Resonant
Mediated- Impaired@ left ICA,MA, IAA, ISA, Infra SA
CVS : S1 S2 + ,no murmurs
P/A : Soft and non tender, no organomegaly
CNS: NFD
PROVISIONAL DIAGNOSIS-
Left sided fibrosis (LL> UL) with COPD with 2° infection ? TB with DM- II
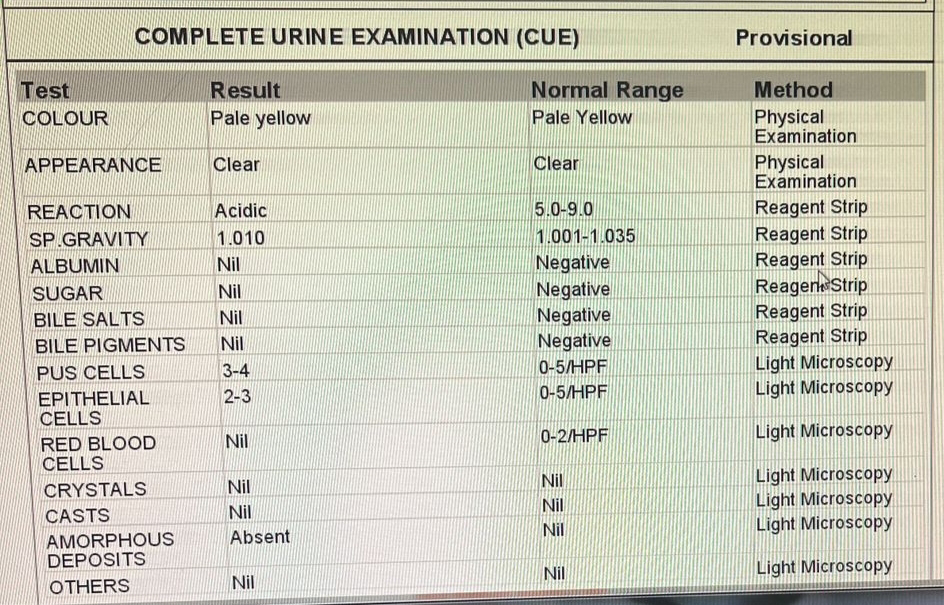
INVESTIGATIONS
2D ECHO
Aortic valve - Sclerotic
No RWMA
EF 60%
Mild to moderate TR with PAH Diastolic dysfunction
HRCT OF THORAX-
Fibrocavitatory changes with traction bronchectasis in both upper lobes with significant volume loss of left lower lobe
Multiple centrilobular nodules in both lungs
Diffuse smooth pleural thickening seen in left costal margin of pleura with few pleural calcification with loculated fluid collection suggestive of fibrothorax/chronic empyema



SPUTUM FOR CULTURE AND SENSITIVITY - POSITIVE
SPUTUM CBNAAT - POSITIVE



























TREATMENT:
ATT(3Tabs) under NTEP BBF
INJ Pan D 40mg iv od bbf
Syp.Grillinctus Dx 2tbsp po tid
Syp. Aptivarte 2tsp po bd
Tab Benadon 20mg po od
Neb with duolin 8th hrly, budecort 12th hrly
T.glimi M1 po after food ( 8am - x - 8pm)
IVF NS @ 500 ML/ HR
GRBS 6TH hrly monitoring
2 egg white/day

Comments
Post a Comment